The following post is a paper written by Maria Null, a junior majoring in Biology, Society, and Environment at the University of Minnesota, in the spring semester of 2015 for Dominique Tobbell’s class HMED 3075. In a recently published pair of articles in the Bulletin of the History of Medicine, Dominique Tobbell and Lois Hendrickson described their use of historical artifacts (from the Wangensteen Historical Library) in their history of medicine courses. Ms. Null’s paper is the second of three papers offered as examples of the work students have done in their classes.
Bandages have demonstrated power as a medical technology in their many varieties, applications, and restorative health qualities throughout the history of humanity. Bandaging as a ‘practice’ has been characterized as an ‘art’ in the literature of medicine, nursing, and mortuary sciences cross-culturally. Notably referred to as a “dying art,” early bandaging has been evidenced by the Egyptian practices of mummification, biblical texts, and popular fictional literature.[1] The prevalence of injuries warranting bandaging in war, medicine, and civilian life are interrelated and their treatments informed by the dissemination of knowledge by those who have studied, practiced, and mastered the “art of bandaging.”
This paper will argue that the improvement of the materials of the triangular bandage, its notable efficacy in sustaining life after being wounded, and the dissemination of its associated knowledge for application during the First World War (1914-1918) contributed to its decline in status as a medical technology through reforms in nursing and ‘first-aid’ education.
“Bandage,” is derived from the French term “bande” meaning an article used to secure an injury and to bind it.[2] It is important, for the purposes of this essay to distinguish between two terms most commonly used interchangeably for one another- “dressing” and “bandage.” In this text, “dressings” will be shortly examined only as they are relevant to the application of a “bandage” to bind the dressing to a portion of the human body. “Bandage” will refer to an apparatus used to either bind a dressing, support a portion of the body, or directly cover a portion of the body during an emergency situation- and in this way, acting as what the reader may mistakenly conceive to be a “dressing.”
The rise of the modern bandage, in its many forms, was coupled by increased knowledge of human anatomy and physiology, which enabled physicians and nurses to designate specific bandages for unique applications to certain portions of the human body. Four unique bandage types have been popularly employed in nursing since the early nineteenth century: the roller bandage, the four-tailed bandage, the scultetus, and the triangular bandage.[3] Each bandage was used for a specific purpose, however each was credited with the capacity to retain dressings or splints.[4] Amongst the four popular bandage types, the late 1800s saw the rise of what became known as the ‘triangular bandage.’ In 1831, Swiss surgeon Mathias Mayor was first credited for acknowledging the utility of what he called the ‘handkerchief bandage.’[5] But the ‘handkerchief bandage’ remained unpopular in medicine until nearly forty years later, when it was used in the field of battle by German surgeon, Professor Johannes Friedrich von Esmarch.[6] In texts and according to manufacturers, Esmarch’s “discovery” defined the triangular bandage throughout the First World War. Indeed, he was the first to suggest printing the illustrations for use, which would come to uniquely characterize the triangular bandage.[7] However, his accomplishment has been contested by medical doctors throughout history due to the leniency with which the triangular bandage may be defined as a technology. [8]
Figure 1. Professor Esmarch’s Bandage with Printed Graphic Illustrating Use
Esmarch’s Bandage: The triangular bandage is depicted with elaborate illustration to inform the user of its many applications.[9] Image captured at the Wangensteen Library.
The triangular bandage as a technology is defined by its existence as a physical object, its versatile functions, and the knowledge needed to apply it.[10] Early nursing texts and supplementary readings suggest the bandage was amorphously fabricated by clothing, linen, pillowcases, handkerchiefs, and bed sheets in dire emergencies. [11] Additional texts inform the physical fabrication and measurements of the technology when bandages were produced to act as a medical technology. Bleached or unbleached muslin or calico, linen, silk, or gauze was utilized in instruction and treatment of injury.[12] The physical measurements of triangular bandages varied and were determined by user selection and eventually by the manufacturer. Texts suggest an appropriate median measurement for the triangular bandage of the 1910s was approximately one square yard.[13] The bandage only serviced its many functions upon folding, which was illustrated in numerous nursing texts and additional ‘first-aid’ handbooks.[14]
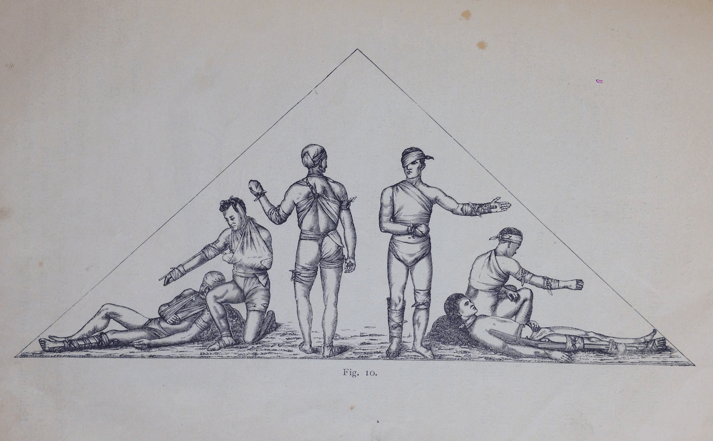
Figure 2. A Manual of Instruction in Folding the Triangular Bandage
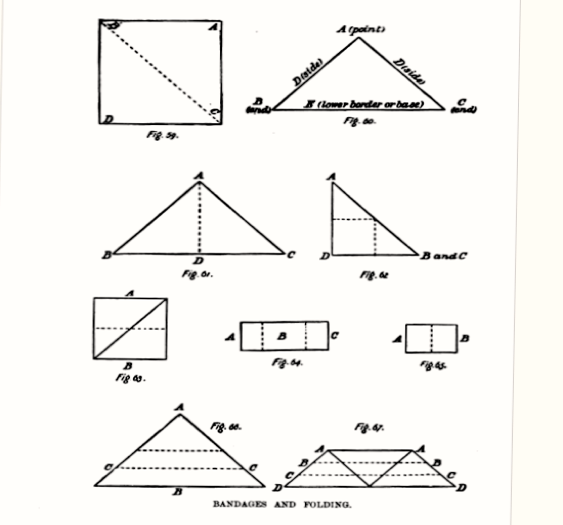
Standard illustration with instructional text in aid book. Figure 59 depicts starting materials, figure 60 the triangular bandage. Figures 61 through 65 depict conversion of the triangular bandage into a compact for storage or transport. Figures 66 and 67 illustrate the folds of the triangular bandage into a ‘cravat’, and subsequent rolling into its ‘cord’ form.[15]
Among its many functions, arresting hemorrhaging was of particular importance in the field of battle- a function requiring extensive knowledge of the many utilities of the triangular bandage for the proper treatment to be achieved. After its introduction to ambulance work in the field by Esmarch in the late 1800s, physicians began producing texts characterized by elaborate illustration and in-depth instruction on triangular bandaging.[16] Understanding texts from the late 1800s through the mid-1920s required knowledge of medical terminology and anatomy, as well as the motivation to learn and practice countless variations on the bandaging techniques. Knowledge of the most useful materials and the speed, neatness, and proper tension required of the application were integral to the success of the treatment, and often the survival of the patient. As the U.S. entered into the First World War, few collective groups in America possessed the same drive and commitment to establishing the agency of the triangular bandage overseas as the United States Army Nursing Corps.
Nurses, patients, first responders, and surgeons observed and experienced the impact of the triangular bandage in medical practice. As a bandage with the primary purpose of serving in emergency situations, first responders were typical users. First responders in the field of battle were soldiers of the U.S. army who were equipped with the bandage in early ‘first-aid kits.’ A ‘first-aider’ as defined by Major Charles Lynch of the Medical Corps of the U.S. Army, was any individual intervening during a medical emergency prior to the summoning or arrival of a physician. [17] Field hospitals stocked with nurses were frontlines of ‘first-aid.’ Triage and dressing stations saw casualties, and upon assessment, nurses donned soldiers with more elaborate triangular bandages. Bandages in field hospitals were not themselves any more complex in fabrication than their field ‘first-aid’ counterparts but they were, however, embodied with greater power to treat injury by the nurses with the knowledge and experience of manipulating them. By 1917 the national curriculum for nursing education had outlined coursework for instruction in the use of the triangular bandage. Elementary bandaging was instructed throughout five classes over a time span of ten hours. Instructors or “competent” head-nurses in association with surgery, orthopedics, and first-aid taught classes. The emphasis on critical manipulation, practice, and demonstration of bandaging skills required speed, efficiency and dexterity of nurses. Likely, two or fewer hours were spent on instruction of the triangular bandage- which was acknowledged as a first aid utility requiring additional education and training.[18] An additional ten hours of instruction on elementary nursing and first aid focused on preparing nurses to adapt readily to emergency situations, much like those in the army. The outline of curriculum emphasized the additional training of nurses required of them upon entry into the Army Nursing Corps.[19]
The evolution of the triangular bandage, in its fabrication and dimensions, contributed to its increasingly widespread use, manufacturing, and distribution to civilians. While the bandage was readily available to any user with the knowledge of textiles, which could be manipulated for bandaging purposes, it was not until the mass production of the ‘Esmarch bandage’ by American consumer healthcare company Johnson & Johnson that civilians saw standard triangular bandages in their very own ‘First-Aid Kits.’ By 1917, Johnson & Johnson was regularly producing a triangular bandage for civilian ‘First-Aid Kits.’[20] The 36 inch squared ‘Esmarch Bandage,’ was a staple of Kits, originally supplied to soldiers as early as the Spanish American war in the late 1800s, when the company had first entered into war-time production efforts.[21] In notes on manufacturing for the American Red Cross, Johnson & Johnson included an “explanation of numbers shown on figures in illustration of the Esmarch Bandage.”[22] The graphic illustration attempted to recreate the iconic print characteristic of Professor Esmarch’s original fabrications. The widespread development and distribution of the bandage extended the user base and established a market for American consumers of first-aid products.
Figure 3. Johnson & Johnson’s Manufactured “Esmarch Bandage”

Johnson & Johnson’s triangular bandage named for Professor Esmarch of Kiel. The bandage mimiced Esmarch’s original design with graphic illustration for the dissemination of knowledge of the bandage’s utilities.[23]
Bandages for purchase were fabricated from surgical gauze or muslin and were available at drug stores. Not only were they staples of the ‘First-Aid Kit,’ but they were also included in the ‘Johnson’s First Aid Cabinet,’ and the popular packet known as ‘Johnson’s First Aid for Wounds.’[24] Both were features of aid in the railroad industry, manufacturing establishments, and schools. The importance of ‘first-aid,’ and responsibility of citizens to learn about it and administer it was demonstrated in Johnson’s First Aid Manual. The manual depicted improved bandaging materials and denounced the improvisation of triangular bandages; in effect suggesting that efficacy of treatment required the newer and standardized ‘first-aid’ materials supplied by the manufacturer.[25]
Indeed, Johnson & Johnson boasted the efficacy of the triangular bandage suggesting, “It is probable no other system of wound dressing can accomplish so much, and in such a reliable manner, in rendering first aid, as the use of the triangular bandage.[26] Improved function with the use of the triangular bandage coupled its improved materials. As the bandage was developed, altered in size to be more compact, and its materials made to be more durable, ‘first-aid’ was rendered more successfully by soldiers, nurses, and civilians. This was demonstrated in part by curriculum change in nursing from 1917 to 1933, which incorporated the new text published by Instructor of Surgery at the University of Pennsylvania, A.D. Whiting: Bandaging. In his text Whiting outlined the effect of the elimination of gauze from use as a fabric for the triangular bandage. While gauze had been a central fabric to earlier triangular bandages, Whiting proclaimed the improved treatment of injury achieved by bandages made of different fabric. Whiting suggested that gauze was not sturdy enough to exercise the utilities of the bandage, and rather bleached or unbleached muslin had been proven materials for increasing proper bandaging and sustaining life in emergency situations.[27] Whiting’s text became the standard for bandaging in nursing curriculum following the First World War and represented the transforming identity of the bandage in several key ways.
While the medical terminology in Whiting’s text maintained the integrity of the triangular bandage as a medical technology within the surgical and nursing professions (including the ‘Occipitofrontal Triangle,’ the ‘Iliofemoral Triangle,’ and the ‘Mentovertico-occipital Cravat), American citizens in the 1910s and 20s were increasingly exposed to new language in popularized ‘first-aid’ education.[28] Johnson & Johnson not only served as a manufacturer contributing to the physical evolution of the triangular bandage, but they also served as a primary source of education on the procedures of ‘first-aid’ as given with their products. Johnson’s First Aid Manual, in its many additions, used language contradictory to that of Whiting’s and other medical texts in the early 1910s. A 1917 edition of Johnson’s explicitly stated, “no instructions are given in this Manual in respect to anatomy or physiology. A knowledge of these subjects is not deemed essential either to the intelligent use of the manual or the application of first aid.”[29] The certainty with which the Manual discerned “non-essential” features of medicine in ‘first-aid’ contributed to a shifting paradigm in U.S. ‘first-aid’ culture. With the improvement of the bandage nearing the end of the First World War, manufacturers, educators, and the American Red Cross began to simplify and consolidate aid education to promote the identity of the ‘first-aider.’
In early texts, the complexity of the triangular bandage as a technology is evident. While the triangular bandage was free in form, it was manipulated by adhering to the principles of geometry. Rudimentary knowledge of the subject was required of users who were instructed to fold the triangular bandage relative to its features: bases, sides, apexes, squares, quadrilaterals, triangles within larger triangles, extremities and ends, and angles of the triangle.[30] ‘Broad’ and ‘narrow’ folds of the bandage and its shape as a ‘cravat’ and ‘cord’ classified its many configurations.[31] Efficacy of the treatment and preservation of life required knowledge of each of these features. Additionally, knowledge of how and where to apply a bandage, and with certain pressure, was essential. A majority of texts alluded to the error, which would result from applying a triangular bandage ineffectively, resulting in the continuity of hemorrhaging or arresting of circulation. While it was often assumed that any attempt at immediate aid (erroneous or informed) would increase chances of survival, texts and aid books asserted that an improperly applied bandage could just as likely harm a patient as hurt them.[32] Extensive study, and practice manipulating the triangular bandage was required of nurses to master the ‘art of bandaging.’ While acknowledging the excessive skill possessed by nurses who “perfected” the “art” of application of the triangular bandage in ‘first-aid,’ virtually no texts awarded them with prestige. This reflects the position of the status in the historical context- nurses characterized by tasks of manual dexterity requiring little subjective analysis of procedures.[33] The bandage itself, in contrast, had reached a new status as an efficacious medical technology as its ‘first-aid’ properties were realized by American civilians following the First World War.
The distribution of knowledge of the bandage to civilians was characterized by a change in the language of texts, illustrations and photographs and demonstrations, and conceptualization of the status of the bandage as a technology. From descriptions of nearly twenty specialized triangular bandages in medical texts such as Whiting’s, to only eight in First Aid in Emergencies, the triangular bandage experienced a reduction in its versatility once adopted by the civilian ‘first-aider.’[34] Fewer varieties of the triangular bandage were included in texts intended for civilian education in aid. Texts, which once required understanding of medical terminology, anatomy, and geometry, were modified for the American consumer. While highly descriptive texts instructed bandaging in the late 1800s, the 1910s saw the efficient integration of photographs with fewer lengthy text inserts. Willing civilians could learn by following step-by-step depictions of bandaging, featured in numerous publications at the time. In her Illustrations of Bandaging and First-Aid, registered nurse Lois Oakes produced knowledge for the public eye- once reserved for the production and consumption by surgeons and nurses. Oakes’ publication thoroughly depicted the many functions of the triangular bandage, attempting to preserve its status as a complex technology. The illustrations and review by the American Journal of Nursing, however, reflected the declining status of the bandage and the popular assumption that any willing individual could become skilled in administering aid.[35] The journal’s review proclaimed Oakes illustrated the use of the bandage “so plainly that even an inexperienced person could study them with advantage.”[36] While not declaring the civilian’s capacity to supersede the skills of a trained nurse, the journal was suggesting that the civilian could acquire the skills once reserved for nurses. Additionally, demonstrations and lectures on first-aid, known as “ambulance” work, became popularized with the public through the American Red Cross several years into the First World War. A 1917 article in the Washington Post reflected varieties of newspaper clips from the time period: lectures on first aid and bandaging for the public.[37] These changes reflected the American attitude toward ‘first-aid’ by the end of the war- that the civilian had the agency and responsibility to become a competent first-aid responder.
Through evident changes in nursing education and ‘first-aid’ curriculum adoption, it is possible to examine the affects the evolution of the triangular bandage ultimately had on its own declining status as a medical technology. While the bandage was increasingly manufactured to meet consumer demand in a new age of civilian ‘first-aid,’ a job that had once formally belonged to a nurse, underwent scrutiny. Updates to the national curriculum in nursing by 1933 reflected a subtle but important decline in time dedicated to bandaging training. Course time in elementary bandaging had been decreased from 10 to eight hours of instruction.[38] In contrast, however, there was a five-hour increase in emergency nursing and first aid. This increase in instructional training (following increased demand following the First World War) might have reflected increased emphasis on emergency bandaging techniques, had the triangular bandage maintained its status as a medical technology. Rather, the opposite occurred. Coursework objectives outlined Army and Red Cross nursing equipment training, training on wounds, fractures, and strains, with no explicit mention of bandaging.[39] Red Cross texts listed as supplementary materials suggest a shift in American aid culture as the U.S. affiliate of the International Federation of the Red Cross and Red Crescent Societies was officially integrated into American nursing education. The motivation of the American Red Cross in aid education was continuously transformed as America adopted ‘first-aid’ culture after the triangular bandage was made accessible. Educating citizens was not only a public health measure, but also a market move in conjunction with consumer healthcare company Johnson & Johnson. The triangular bandage and its manual in the ‘First-Aid Kit’ of the home, the factory, and the school empowered citizens and subsequently lowered its status as a medical technology in the hands of the educated, practiced, and masterfully skilled artists of bandaging: America’s nurses.
Gradually, references to the Esmarch bandage began to disappear from texts by the 1940s. Due in part to the emergence of newer technologies (some developed by Esmarch himself, including a rubber bandage), but largely determined by declining status as a medical technology, the complexity of the triangular bandage fell out of favor with clinical and civilian texts. Many outside actors had established the importance of first-aid, namely, manufacturer Johnson & Johnson backed by the American Red Cross. The ‘art of bandaging’ so masterfully executed by trained nurses was simplified and condensed to teach the civilian to adopt the new identity of the American ‘first-aider’: an obligated responder in emergency situations. The relegation of the triangular bandage largely contributed to its disappearance as a prominent feature of nursing curriculum. However, the change was successful in establishing a solid foundation of ‘first-aid’ for American citizens. From a soldier’s pocket to the nurse’s field hospital to the hands of the American adolescent in ‘first-aid’ class, the triangular bandage was one of the most versatile medical technologies to ever reach the hands of the American citizen.
[1] Herrmann, E.K. “The Dying Art of Bandaging,” Western Journal of Nursing Research Vol. 14, No.6 (1992): 791.
[2] Ambulance Work and Nursing (Chicago: W. T. Keener & Co., 1899), 67.
[3] Committee on Education of the National League of Nursing Education, Standard Curriculum for Schools of Nursing. (Baltimore: Waverly Press,1917), 86.
[4] Albert S. Marrow, The Immediate Care of the Injured (Philadelphia and London: W.B. Saunders Company, 1906), 108.
[5] Little, Vincent J. “The Fabric of First Aid: A History of the Triangular Bandage.” Pharmacy History Australia: The Newsletter of the Australian Academy for the History of Pharmacy no.9 (1999): 10.
[6] Ibid
[7] Ambulance Work, 67.
[8] J.M. Grant M.D. “Professor Esmarch’s Triangular Bandage,” The Lancet (1874): 746.
[9] Johannes Friedreich von Esmarch, Samariterbriefe (Kiel: Verlag von Lipsius & Tischer, 1886), 29.
[10] Joel D. Howell, Technology in the Hospital: Transforming Patient Care in the
Early Twentieth Century (Baltimore: Johns Hopkins University Press, 1995), 8.
[11] Major Charles Lynch, American Red Cross Abridged Text-Book on First Aid: Women’s Addition; a Manual of Instruction (Philadelphia: P. Blakiston’s Son & Co., 1913), 10; Alvah H. Doty, M.D., A Manual of Instruction in Principles of Prompt Aid to the Injured: Designed for Military and Civil Use (New York: D. Appleton and Company, 1890), 77.
[12] Henry R. Wharton, M.D., Minor Surgery and Bandaging (Philadelphia and New York: Lea Brothers & Co., 1902), 17.
[13] Albert S. Marrow, The Immediate Care of the Injured, 134.
[14] Ambulance Work, 68.
[15] Ibid
[16] Henry C. Leonard, A Manual of Bandaging: Adapted for Self-Instruction. (Detroit: Daily Post Book Printing Establishment, 1876).
[17] Lynch, Charles, American Red Cross Abridged, 2.
[18] Committee on Education. Standard Curriculum for Schools of Nursing, 85.
[19] Committee on Education. Standard Curriculum for Schools of Nursing, 117.
[20] W.G. Stimpson. Prevention of Disease and Care of the Sick, (Washington: Government Printing Office, 1917), 224.
[21] Ibid;General Index to Red Cross Notes, (New Brunswick: Johnson & Johnson, 1900), 18.
[22] General Index to Red Cross Notes, 104.
[23] A.D. Whiting, Bandaging, (Philadelphia and London: W. B. Saunders Company, 1915), 131.
[24] Johnson’s First Aid Manual, (Baltimore: Johnson & Johnson, 1917), 59.
[25] Johnson’s First Aid Manual, 69-75.
[26] Johnson’s First Aid Manual, 69.
[27] A.D. Whiting, Preface to Bandaging, 7.
[28] A.D. Whiting, Bandaging, 132-143.
[29] Johnson’s First Aid Manual, 3.
[30] Ambulence Work, 68.
[31] Ambulence Work, 69.
[32] Charles Lynch, American Red Cross Abridged, 1.
[33] Dominique Tobbell, “Nursing In the Early 20th Century.” (Lecture presented, Minneapolis, Minnesota, October 05, 2015).
[34] A.D. Whiting, Bandaging, 10; Eldridge L. Eliason, in Contents of First Aid in Emergencies, (Philadelphia and London: J.B. Lincott Company, 1915), v.
[35] Lois Oakes. Illustrations of Bandaging and First-Aid (Baltimore: The Williams and Wilkins Company, 1942).
[36] “Book Reviews” American Journal of Nursing. Vol 41, No. 1 (1941): 130.
[37] “First Aid Advice in Red Cross Lecture,” Washington Post, March 22nd, 1917, 4.
[38] Committee on Education of the National League of Nursing Education, A Curriculum for Schools of Nursing, (New York: National League of Nursing Education, 1932), 108.
[39] Committee on Education , A Curriculum, 155.
